

Most people who smoke know about the risks to the heart and lungs. Far fewer know what tobacco does to the eyes. The link between smoking and eye disease is one of the strongest and most repeatedly proven in all of eye medicine, and it follows a clear pattern: the more someone smokes, and the longer they smoke for, the greater the harm.
Smoking is the most important avoidable risk factor for age-related macular degeneration (AMD), the leading cause of severe sight loss in older adults in the UK. It also speeds up cataracts, worsens dry eye, and is linked to a higher risk of several other eye conditions. These are not vague warnings. They translate into vision lost earlier in life, cataract surgery needed sooner, and in the worst cases central vision damage that no amount of surgical skill can undo.
How Tobacco Reaches and Harms the Eye
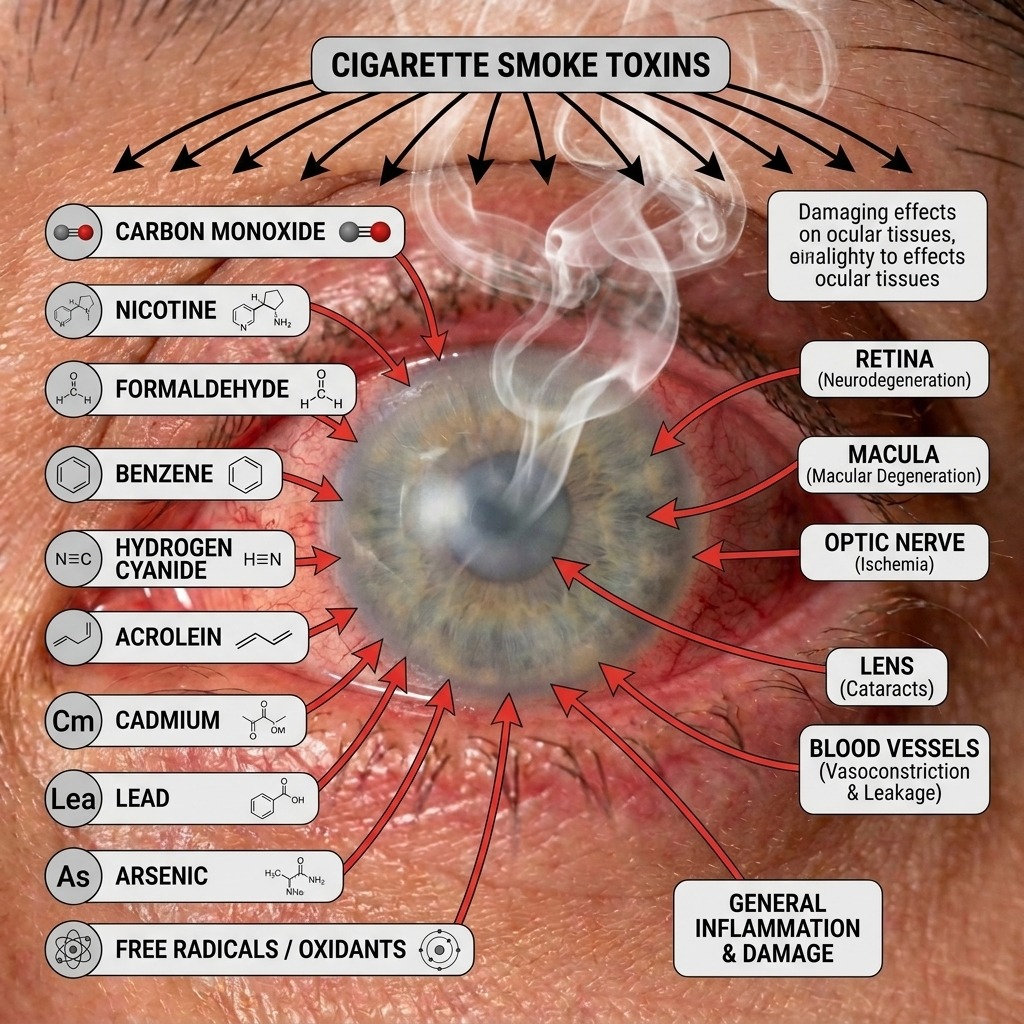
Cigarette smoke contains thousands of different chemicals, many of them toxic and dozens known to cause cancer. Several of these harm the eye at the same time, through three main routes.
Oxidative stress. The retina is one of the busiest, most oxygen-hungry tissues in the body, which makes it very sensitive to chemical wear and tear. Smoke floods the eye with unstable molecules called free radicals that overwhelm its natural defences. Over years, this damages the retinal pigment epithelium, a layer of support cells beneath the retina, and this is part of how AMD develops.
Reduced blood flow. Nicotine narrows blood vessels, which cuts the blood supply to the choroid, the vessel-rich layer that feeds the retina. Carbon monoxide in smoke also lowers how much oxygen the blood can carry. Together this starves delicate tissues of oxygen, and the same vessel damage helps cataracts form faster.
Inflammation. Smoking pushes the whole body into a low-grade inflamed state. In the eye, this is linked to a higher risk of uveitis (inflammation inside the eye) and to worse dry eye, with a less stable tear film and more inflammatory signals in the tears.
Macular Degeneration: The Strongest Link of All
The connection between smoking and AMD is one of the best-established findings in eye research. Studies consistently show that current smokers have roughly three to four times the risk of developing advanced AMD compared with people who have never smoked. The risk depends on the dose: the more someone has smoked over their life, the higher it climbs.
AMD affects the macula, the central part of the retina used for reading, recognising faces, and any fine detail. In its advanced stages it takes two forms. In dry AMD, the central cells slowly waste away over years. In wet AMD, fragile new blood vessels grow under the retina and leak fluid or blood, which can damage central vision quickly.
Wet AMD can be treated with injections into the eye that protect sight, and they work well when started promptly. But most people need these injections regularly for years to hold on to the vision they have. The simple message is that stopping smoking does more to lower AMD risk than any supplement, drug or operation.
Cataracts: Clouding That Arrives Sooner
The eye's lens stays clear thanks to neatly arranged proteins and a careful antioxidant balance. Smoking upsets both. A toxic metal called cadmium, found in tobacco smoke, builds up in the lens; the smoke drains the lens of its natural protective chemicals; and poorer blood supply starves it of nutrients.
The result is cataracts that form earlier. Large reviews show that heavy smokers are roughly two to three times more likely to develop a nuclear cataract, the most common type, and these cataracts tend to be denser by the time they are found. Cataract surgery is safe and effective when the time comes, but avoiding an earlier operation by not smoking is clearly the better path.
Dry Eye: A Surface Under Constant Attack
Dry eye is more common, and often more severe, in people who smoke. Smoke particles irritate the surface cells that make the watery and mucus parts of tears, disturb the eyelid oil glands that stop tears evaporating, and affect the tear-producing gland itself.
The outcome is a tear film that is unstable and does not protect the eye well, leading to burning, redness, watering, grittiness and light sensitivity. For people already prone to dry eyes, including those living in busy urban areas where air quality plays a part, smoking adds a heavy extra load.
The Wider Picture: Uveitis, Optic Nerve and Diabetes
Beyond AMD, cataract and dry eye, smoking is linked to several other problems worth knowing about.
Uveitis: smokers have a higher risk of this inflammation inside the eye, and it tends to come back more often and be harder to settle.
Optic nerve damage: the effects of smoking on small blood vessels raise the risk of a sudden loss of blood supply to the optic nerve, which can cause permanent vision loss in one eye.
Diabetic eye disease: for people with diabetes, smoking markedly speeds up damage to the retina's blood vessels. Here, stopping smoking is not just lifestyle advice, it is an important part of protecting sight.
There is also a strong link with thyroid eye disease, a condition affecting the tissues around the eye. Smoking makes it more severe and harder to treat, and stopping is one of the most useful things a patient can do.
What Changes When You Stop
The encouraging part of this story is that much of the risk is reversible, and some of it quite quickly. Dry eye symptoms often ease within weeks to months of stopping. AMD risk begins to fall after quitting, although it takes years of being smoke-free to get close to a never-smoker's level. Existing cataract or scarring will not undo itself, but stopping slows down further damage.
Quitting is genuinely hard, because nicotine is strongly addictive, and most people need several attempts. In the UK, free NHS Stop Smoking services, available through GP practices and pharmacies, offer support and treatments such as nicotine replacement and prescription medicines, which together greatly improve the chances of stopping for good. Your GP or pharmacist can advise on which options are currently available and suitable for you.
Bringing It Together
If you smoke and are being seen for AMD monitoring, a cataract assessment or dry eye, stopping should be part of the conversation about your care. It is the single most evidence-based step an eye specialist can recommend for protecting your sight in the long term. If you have noticed any change in your vision, it is also worth having an assessment so you know where things stand.
References
- Thornton J, Edwards R, Mitchell P, Harrison RA, Buchan I, Kelly SP. Smoking and age-related macular degeneration: a review of association. Eye (Lond). 2005;19(9):935–944.
- Chakravarthy U, Wong TY, Fletcher A, et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10:31.
- National Institute for Health and Care Excellence. Age-related macular degeneration. NICE Guideline NG82. London: NICE; 2018.
- Cheng ACK, Pang CP, Leung ATS, Chua JKH, Fan DSP, Lam DSC. The association between cigarette smoking and ocular diseases. Hong Kong Med J. 2000;6(2):195–202.
- Ye J, He J, Wang C, et al. Smoking and risk of age-related cataract: a meta-analysis. Invest Ophthalmol Vis Sci. 2012;53(7):3885–3895.
- Tear Film and Ocular Surface Society. TFOS DEWS III Report. The Ocular Surface; 2025.
- Vessey MP, Villard-Mackintosh L, McPherson K, Yeates D. Oral contraceptives, smoking and other factors in relation to uveitis. Br J Ophthalmol. 1990 (and subsequent cohort analyses).
- Thornton J, Kelly SP, Harrison RA, Edwards R. Cigarette smoking and thyroid eye disease: a systematic review. Eye (Lond). 2007;21(9):1135–1145.
- National Institute for Health and Care Excellence. Tobacco: preventing uptake, promoting quitting and treating dependence. NICE Guideline NG209. London: NICE; 2021.
- Royal College of Ophthalmologists. Age-Related Macular Degeneration: Guidelines for Management. London: RCOphth; 2013.
