
Getting something in your eye is one of the most common reasons people attend an emergency eye clinic, and the reassuring news is that most cases are sorted out quickly and heal well. A speck of grit, a tiny flake of metal from grinding, a splinter of wood, a chip of glass, or even the rough edge of a contact lens can all end up on the surface of the eye. What happens next depends on three things: what the object is made of, how deep it has gone, and how soon it is examined properly.
This article explains what a foreign body in the eye actually is, how it should be assessed, what treatment involves, what recovery feels like, and the warning signs that mean an eye needs to be seen straight away.
Not every "something in the eye" is the same
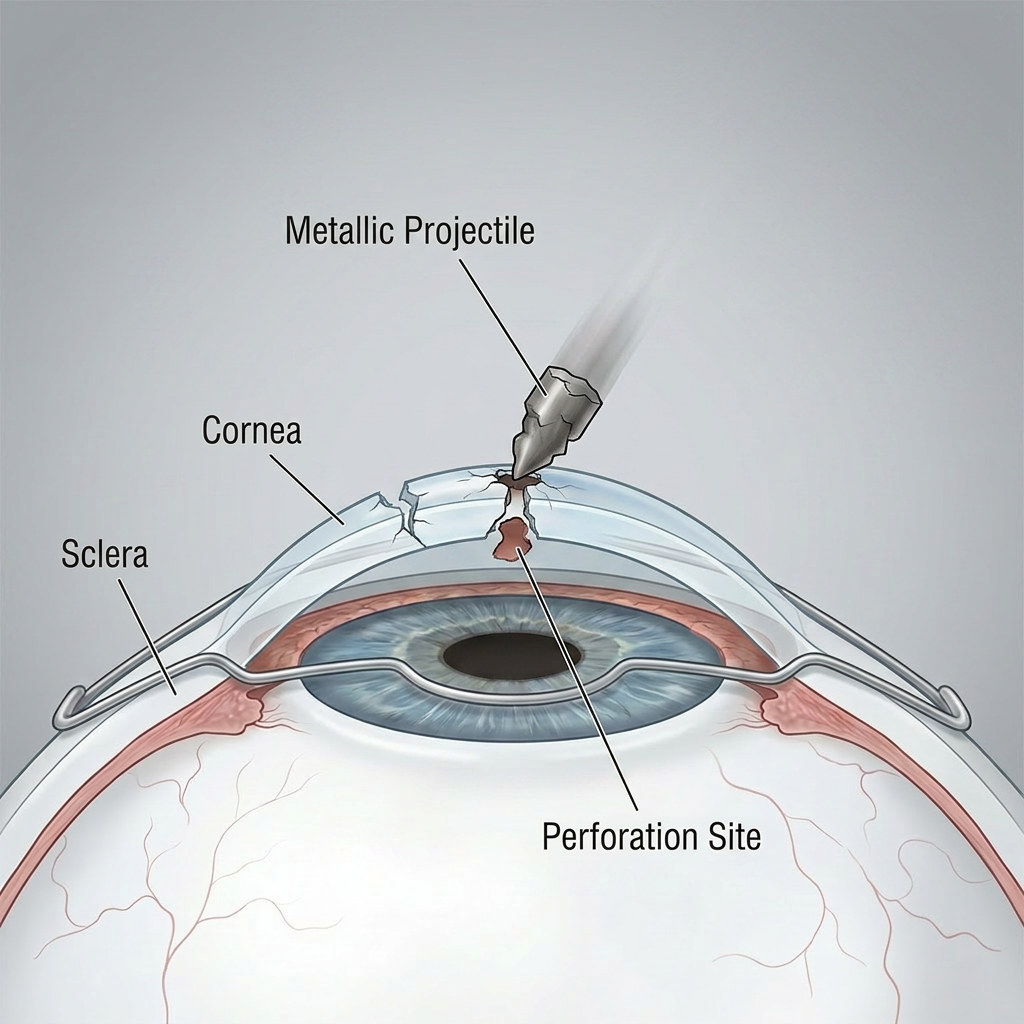
Doctors use the term foreign body for anything that lands on or in the eye from outside. Where it sits matters a great deal. A superficial foreign body rests on the clear front window of the eye, the cornea, without going deep. A subtarsal foreign body hides under the upper eyelid and scratches the cornea with every blink, leaving fine vertical lines on the surface. A deeply embedded foreign body pushes into the middle layer of the cornea. The most serious type, an intraocular foreign body, breaks through the outer wall of the eye and travels inside it.
This is why two people who both say they have "something in the eye" can need completely different care. A surface speck might be lifted off in a couple of minutes. A fragment that has gone inside the eye is an emergency.
Why what it is made of matters as much as where it is
The material is just as important as the location. Bits of plant or wood carry a real risk of infection and need prompt attention. Iron-containing metal behaves differently again: once it has been sitting in the cornea for a few hours, it starts to rust, leaving a brown "rust ring" of damaged tissue around the fragment. If this ring is left behind, it can keep the eye inflamed and may leave a small scar. Glass is usually harmless to the tissue itself but can be surprisingly hard to spot without a careful examination using a microscope called a slit lamp.
A foreign body is also not the same as a corneal abrasion, which is a simple scratch with nothing left behind, although the two often happen together. Telling them apart changes the treatment, which is one reason an unhurried look matters.
How a foreign body should be checked
A good assessment starts with a few simple questions: what were you doing, and what hit the eye? High-speed metal-on-metal work, such as hammering or grinding without eye protection, is the classic way a fragment can pierce the eye and lodge inside it.¹ When that history is present, the eye is examined closely and a CT scan may be needed to make sure nothing is sitting inside the globe. The upper lid is usually turned back to check underneath, the surface is stained with a harmless dye to reveal scratches, and the vision is recorded. None of this is uncomfortable beyond the initial irritation.
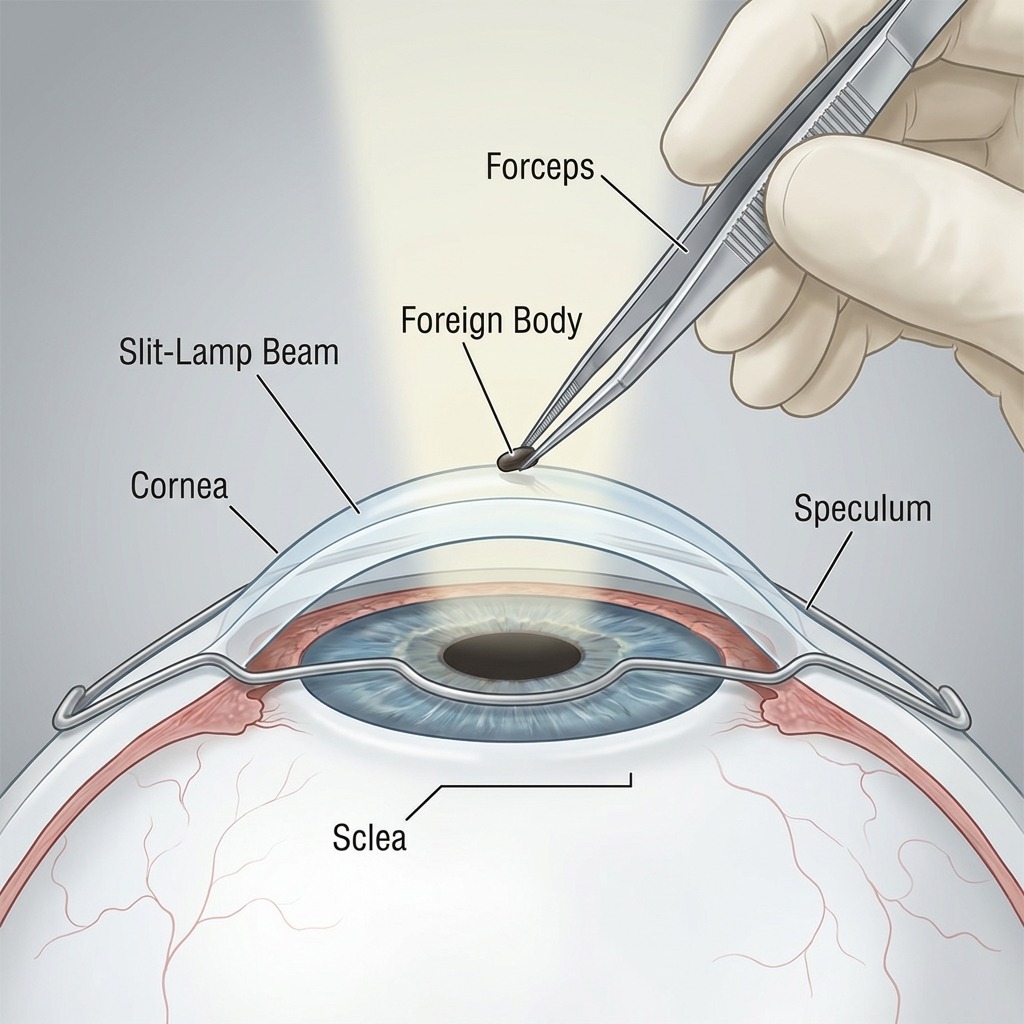
Getting it out safely
Most surface foreign bodies are removed there and then at the slit lamp. Numbing drops make the eye comfortable, and the fragment is lifted off with a fine sterile needle, or a small rotating burr if there is rust. The whole thing usually takes only a few minutes and does not need an operating theatre.
The theatre is kept for the minority of cases: fragments that have gone deep, suspected or confirmed penetrating injuries, and young children who cannot stay still for such a delicate procedure. There, with full magnification and the right instruments, any wound can be repaired and the inside of the eye protected.
When a rust ring has formed, there is a genuine choice to make. Sometimes it is best removed at the same sitting; at other times it is gentler to use antibiotic drops and lift the softened ring a day or two later. Both approaches are reasonable, and a careful clinician will explain which one they are choosing and why.² What matters most is that the rust is fully cleared and the surface is allowed to heal.
What recovery feels like
Recovery is usually quick, but not instant. A small surface defect normally heals within one to three days. During that time the eye often feels gritty, watery and sensitive to light. Many people are surprised that the first 12 to 24 hours after removal can feel worse than the foreign body did. This is normal as the numbing drops wear off and the surface knits back together. Antibiotic drops are usually given to lower the risk of infection, and lubricating drops help the surface settle.²
Problems that can hide behind an eye injury
An injury sometimes brings other issues to light. Keratoconus, in which the cornea slowly thins and bulges into a cone shape, can blur vision in a way that glasses cannot fully correct. Caught early, a treatment called corneal crosslinking can slow or stop it getting worse in many people. Dry eye disease is another. The 2025 TFOS DEWS III report describes it as a condition in which the tear film and the surface of the eye lose their natural balance, leading to inflammation and discomfort. A dry, inflamed surface tends to heal more slowly after an injury, so it is worth mentioning any long-standing burning, grittiness or fluctuating vision at your appointment.
When to treat it as an emergency
Seek urgent care the same day if the eye was struck by a high-speed fragment, if your vision has dropped, if there is significant pain or light sensitivity, if there is a visible cut on the eye, or if chemicals were involved. Above all, do not rub the eye. Rubbing can drive a fragment deeper or worsen a wound that is not yet obvious.¹
The reassuring reality
The large majority of foreign body injuries are minor and heal completely with prompt, careful treatment. Knowing the warning signs, protecting your eyes during risky work, and having an unhurried, thorough examination when something does go wrong are the things that keep the outcome a good one.
References
- Royal College of Ophthalmologists. Ophthalmic Services Guidance: The Management of Ophthalmic Trauma. London: RCOphth; 2024.
- National Institute for Health and Care Excellence. Corneal superficial injury. Clinical Knowledge Summaries. London: NICE; 2024.
- American Academy of Ophthalmology. Corneal Foreign Body. San Francisco: AAO; 2023.
- Wipperman JL, Dorsch JN. Evaluation and management of corneal abrasions. American Family Physician. 2013;87(2):114–120.
- Sykakis E, Karim R, Evans JR, et al. Corneal collagen cross-linking for treating keratoconus. Cochrane Database of Systematic Reviews. 2015;(3):CD010621.
- National Institute for Health and Care Excellence. Photochemical corneal collagen cross-linkage using riboflavin and ultraviolet A for keratoconus and keratectasia. Interventional Procedures Guidance IPG466. London: NICE; 2013.
- Wolffsohn JS, Craig JP, Stapleton F, et al. TFOS DEWS III: Diagnostic Methodology and Executive Summary. American Journal of Ophthalmology. 2025.
