
Few things unsettle a parent more than being told that something is changing inside their child’s eye. Keratoconus is one of those conditions that can sound frightening at first, yet it is far more manageable today than it once was. Understanding what it is, why it tends to appear during the teenage years, and what can be done about it will help you support your child calmly and make good decisions together.
What keratoconus actually is
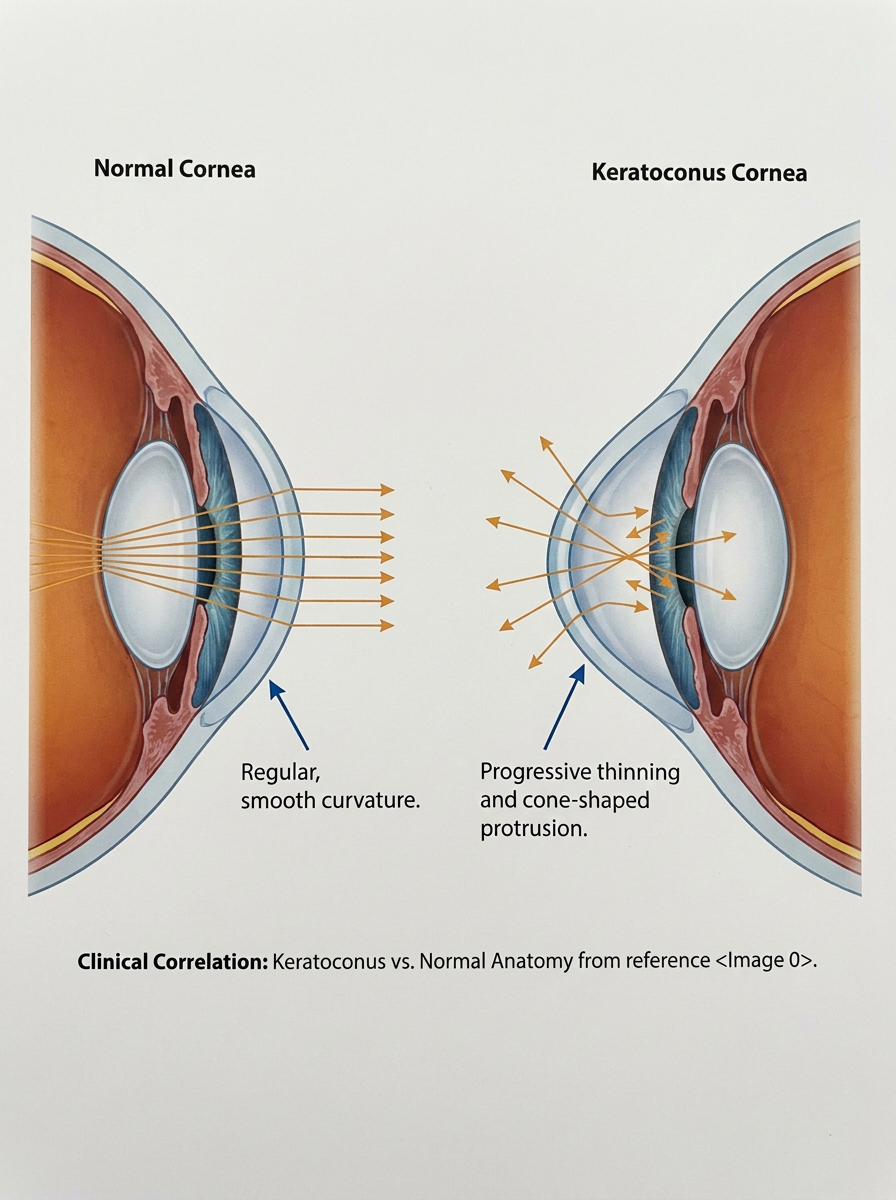
The cornea is the clear, curved window at the front of the eye. It behaves a little like a camera lens, bending light so that a sharp picture lands at the back of the eye. In keratoconus, the cornea slowly becomes thinner and weaker, and instead of holding its smooth dome shape it begins to bulge outwards into a cone. Because the surface is no longer even, light scatters rather than focusing cleanly, and vision turns blurred or distorted. This is sometimes called irregular astigmatism, which simply means the front of the eye has an uneven shape that ordinary glasses cannot fully correct.
Why it tends to appear in the teenage years
Keratoconus usually shows itself around puberty and slowly progresses over the years that follow. This timing is not a coincidence. The young cornea is softer and more flexible, and the condition tends to be more active and faster moving in teenagers than in adults. It is also more common than once believed. Older figures suggested it affected roughly one in 1,750 people, but detailed scanning of the cornea now picks up milder cases that were previously missed.
What raises the risk
Several things make keratoconus more likely. Family history matters, so if a parent or sibling has it, the chance is higher. The habit most worth knowing about is eye rubbing. Hard, repeated rubbing places mechanical stress on an already weakened cornea and can speed the condition along.
Rubbing is often driven by allergies, and conditions such as eczema, asthma and hay fever are seen more often in children who develop keratoconus. A few genetic conditions, including Down’s syndrome, also carry a higher risk. Treating allergies well and gently discouraging eye rubbing are simple, practical steps that genuinely help.
The signs parents might notice
One of the harder things about keratoconus in young people is how quietly it can begin. Children often assume that the way they see is normal, so they rarely complain. The clues a parent may spot include blurring that glasses do not seem to fix, a prescription that keeps changing at every visit, sensitivity to bright light, glare or halos around lights at night, and sometimes a ghosting or smearing of images in one eye. A repeatedly changing astigmatism prescription, in particular, is well worth raising with an optometrist.
How it is diagnosed
A routine eye test is often where the first hint appears. If keratoconus is suspected, the cornea is examined in more detail with a scan called corneal topography, which maps the shape and thickness of the surface rather like a contour map of a hill. These maps can detect the condition early, before vision is badly affected, and they allow the eye to be watched closely over time. Because young eyes can change quickly, review appointments are often arranged every few months rather than once a year.
How it is treated
The reassuring news is that keratoconus is very treatable, and the earlier it is found the more choices there are. In mild cases, glasses or soft contact lenses may give perfectly good vision. As the surface becomes more irregular, specially fitted rigid or scleral contact lenses can sit over the uneven cornea and create a smooth front surface, often restoring clear, comfortable sight.
The most important advance for young patients is a treatment called corneal cross-linking. It uses vitamin B2 drops and a controlled dose of ultraviolet light to form new bonds within the cornea, strengthening it rather than adding scaffolding to a structure. It is currently the only treatment shown to stop keratoconus getting worse, and it halts progression in more than nine out of ten cases. In teenagers with active disease, doing this early is especially valuable, because it can protect the vision they still have before further damage occurs. Treatment is usually carried out on one eye at a time, and it is offered when there is clear evidence that the condition is progressing.
If keratoconus becomes advanced before it is treated, a corneal transplant may eventually be needed, and the condition still accounts for around a quarter of all corneal transplants performed in the UK.
Finding the problem early and strengthening the cornea in good time is how that outcome is increasingly being prevented.
What outcomes parents can realistically expect
Most teenagers with keratoconus go on to lead completely ordinary lives, continuing with school, sport and screens without lasting difficulty. The goal of care is not perfection but stability: protecting the vision your child already has and keeping their future options open. With timely treatment, the great majority keep useful, comfortable sight for the long term.5
When to seek help
If your child squints, mentions blurred or doubled vision, rubs their eyes a great deal, or needs new glasses unusually often, it is worth arranging an eye examination. There is no need for alarm, but there is real value in acting promptly, since the cornea can be stabilised most effectively during these younger years.
Keratoconus in a teenager can feel daunting when you first hear the word, yet it is a condition that modern eye care manages well. Early detection, careful monitoring, sensible allergy control and, where it is needed, cross-linking have together changed what this diagnosis means for young people. With the right support at the right time, your child’s sight can be protected through the years when it matters most.
References
- Royal National Institute of Blind People. Keratoconus. London: RNIB; 2024. Available at: https://www.rnib.org.uk/your-eyes/eye-conditions-az/keratoconus/
- Guy’s and St Thomas’ NHS Foundation Trust. Photochemical corneal collagen cross-linking for keratoconus. London: GSTT; 2023. Available at: https://www.guysandstthomas.nhs.uk/health-information/photochemical-corneal-collagen-cross-linking-keratoconus
- Larkin DFP, Chowdhury K, Burr JM, Raynor M, Edwards M, Tuft SJ, et al. Effect of corneal cross-linking versus standard care on keratoconus progression in young patients (KERALINK): a randomised controlled trial. Ophthalmology. 2021;128(11):1516–1526.
- National Institute for Health and Care Excellence. Photochemical corneal collagen cross-linkage using riboflavin and ultraviolet A for keratoconus and keratectasia. Interventional procedures guidance IPG466 (now HealthTech guidance HTG319). London: NICE; 2013. Available at: https://www.nice.org.uk/guidance/ipg466
- Hull University Teaching Hospitals NHS Trust. Corneal collagen cross-linking (CXL) for keratoconus. Hull: HUTH; 2023. Available at: https://www.hey.nhs.uk/patient-leaflet/corneal-collagen-crosslinking-cxl-for-keratoconus/
- Davidson AE, Hayes S, Hardcastle AJ, Tuft SJ. The pathogenesis of keratoconus. Eye (London). 2014;28(2):189–195.
- Hashemi H, Heydarian S, Hooshmand E, Saatchi M, Yekta A, Aghamirsalim M, et al. The prevalence and risk factors for keratoconus: a systematic review and meta-analysis. Cornea. 2020;39(2):263–270.
