
Have you ever had a pebble in your shoe or a piece of grit in your eye? It hurts, right? Pain is your body’s alarm system, telling you that something is wrong and needs your attention. But what happens if the alarm system never goes off?
When it comes to your eyes, one of the biggest threats operates in total silence. It is a condition called glaucoma, and it is a leading cause of irreversible blindness, affecting over half a million people in the UK alone. The scary part is that for most people with the common type of glaucoma, there is absolutely no pain, and their vision seems perfectly normal until the disease has already done major damage.
What exactly is Glaucoma?
Think of your eye like a water balloon. It is constantly filled with a clear fluid called the aqueous humour. To stop the balloon from overfilling, this fluid is constantly drained away through a tiny, spongy filter inside your eye called the trabecular meshwork. This balancing act keeps your eye perfectly plump and maintains a healthy pressure.
However, in Primary Open Angle Glaucoma (the most common type), that tiny drainage system gets clogged. Because the fluid cannot escape as fast as it is being made, the pressure inside the eye slowly starts to rise.
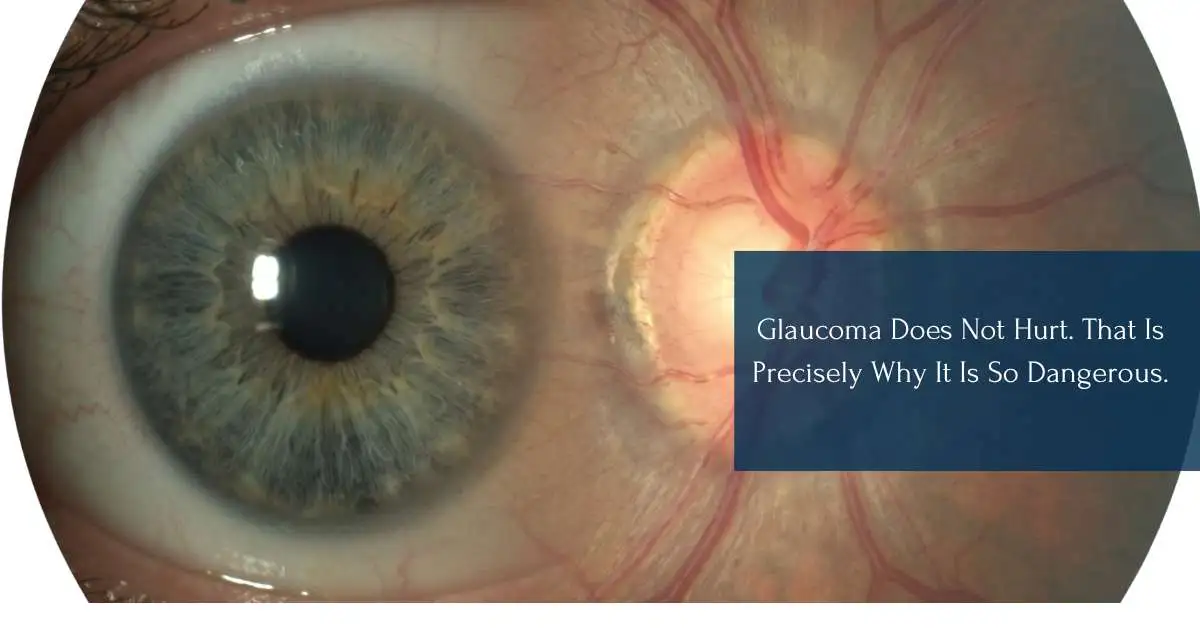
This extra pressure squashes the most delicate part of your eye: the optic nerve. The optic nerve is like a massive fibre-optic cable connecting your eye to your brain. It is made up of millions of tiny wire-like cells called Retinal Ganglion Cells. When the eye pressure gets too high, these sensitive cells slowly die, breaking the connection to the brain.
Why Doesn't It Hurt?
You might wonder how your eye can be under so much pressure without you feeling a thing. The answer is that the rise in pressure happens so incredibly slowly that it does not trigger the pain receptors in your eye. Your body simply gets used to it.
Even worse, you will not notice the vision loss at first. Glaucoma does not usually blur the centre of your vision right away. Instead, it steals your peripheral vision-the things you see out of the extreme corners of your eyes.
Because these changes happen so gradually, your brain plays a trick on you. It takes the information from your healthy central vision and automatically "fills in the gaps" around the edges. By the time a person actually notices that their vision is getting narrower or they start bumping into doors, a huge amount of the optic nerve has already been destroyed.
The Point of No Return
That "silent" nature is exactly why glaucoma is so dangerous. Once the optic nerve is damaged, it cannot be repaired. Any vision that is lost to glaucoma is gone forever. If someone waits until they have trouble reading or watching television to see an eye doctor, it means the disease has already destroyed the vast majority of their retinal ganglion cells, and their sight cannot be brought back.
Catching the Silent Thief
If glaucoma does not hurt and you cannot see it happening, how do you stop it? The answer is simple: regular eye tests.
Even though you cannot feel the pressure building up, an optician or ophthalmologist has special tools to easily measure it. They can also use advanced 3D scanners to look at the very back of your eye, checking the optic nerve for the tiniest signs of damage long before any vision is actually lost.
If glaucoma is caught early, doctors can prescribe special eye drops to lower the pressure and protect your sight. Sometimes, quick laser treatments or surgeries are used to help the fluid drain better. Because the disease hides in the background without giving you any warning signs, it is completely up to us to be proactive. Getting your eyes checked regularly is the only way to make sure the silent thief of sight is stopped in its tracks.
References
- Cohen, L. P., & Pasquale, L. R. (2014). Clinical Characteristics and Current Treatment of Glaucoma. Cold Spring Harbor Perspectives in Medicine, 4, a017236-a017236. https://doi.org/10.1101/cshperspect.a017236
- Elghobashy, M., Lamont, H. C., Morelli-Batters, A., Masood, I., & Hill, L. J. (2022). Magnesium and Its Role in Primary Open Angle Glaucoma; A Novel Therapeutic?. Frontiers in Ophthalmology, 2. https://doi.org/10.3389/fopht.2022.897128
- Harwerth, R. S. (2006). Visual Field Defects and Retinal Ganglion Cell Losses in Patients With Glaucoma. Archives of Ophthalmology, 124, 853. https://doi.org/10.1001/archopht.124.6.853
- Kastner, A., & King, A. J. (2019). Advanced glaucoma at diagnosis: current perspectives. Eye, 34, 116–128. https://doi.org/10.1038/s41433-019-0637-2
- Vandersnickt, M. F., van Eijgen, J., Lemmens, S., Stalmans, I., Pinto, L. A., & Vandewalle, E. M. (2024). Visual field patterns in glaucoma: A systematic review. Saudi Journal of Ophthalmology, 38, 306-315. https://doi.org/10.4103/sjopt.sjopt_143_24
