

Most eye problems are minor and settle on their own. A small number are warning signs that need quick attention, and a few are emergencies where every hour counts. The difficult part is that serious eye conditions do not always feel dramatic at first. Some come on slowly and are easy to brush off. Others appear suddenly, with only a short window in which treatment can protect your sight.
This guide explains seven symptoms that should prompt a check by an eye specialist, and roughly how quickly to act. It is written with people in Leicester and nearby areas such as South Leicester, Narborough, Lutterworth, Warwick and Hinckley in mind, but the advice applies to anyone. None of it replaces a proper examination. The aim is simply to help you recognise when waiting is not a safe option.
1. When the Lights Go Out in One Eye

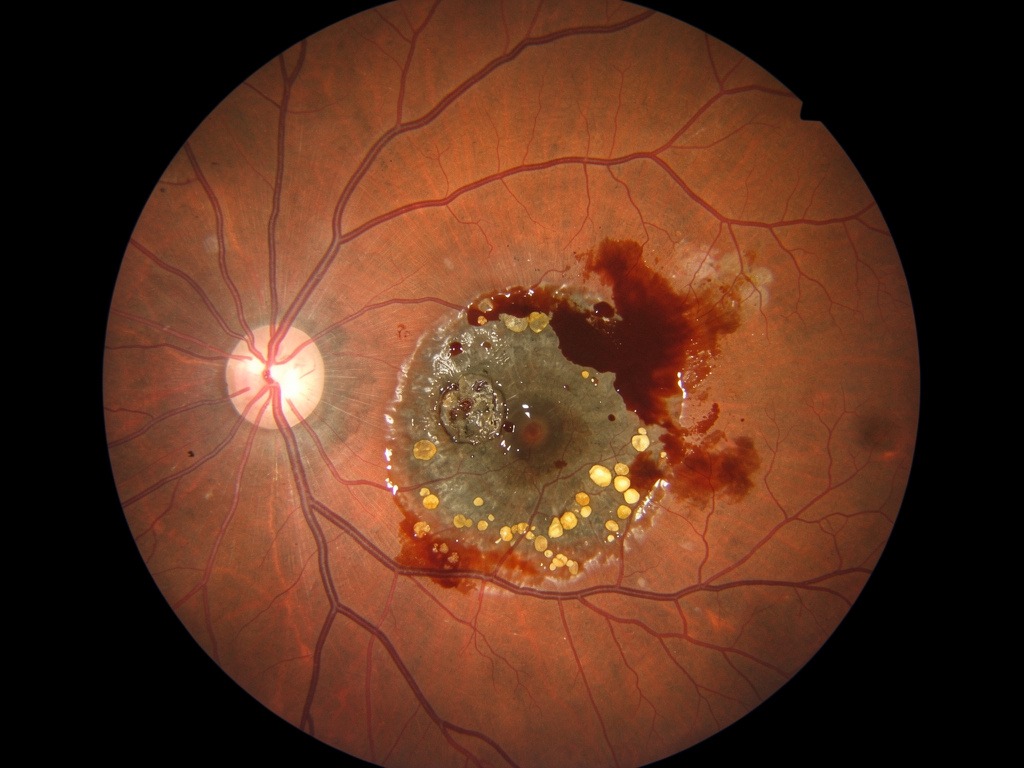
Fig: retinal image of a central retinal artery occlusion. The central red spot is the area of central retina where underlying blood flow is being picked out as the retina has gone pale due to lack of blood circulation.
A sudden, painless loss of vision in one eye is an emergency. People often describe it as a curtain coming down, a dark or grey shadow, or everything simply going dark. If this happens, you need to be seen the same day.
One cause is a central retinal artery occlusion, sometimes called a stroke of the eye, where the main blood vessel to the retina becomes blocked. This kind of event can also be the first sign of a problem with the heart or blood vessels, so it needs urgent medical checks as well as eye care. Another cause, mainly in older adults, is giant cell arteritis, an inflammation of blood vessels that can threaten both eyes if untreated. It is treatable when caught early, usually with steroids started quickly.
What to do: go to an emergency eye service or A&E straight away. Do not wait until the next morning to see your GP.
2. A Sudden Storm of Specks and Sparks
Floaters are the small specks, threads or cobweb shapes that drift across your vision. Floaters you have had for years, which stay much the same, are rarely a cause for concern.
The pattern that needs attention is a sudden change: a new burst of floaters, especially alongside flashes of light at the edge of your vision. This often points to a posterior vitreous detachment, where the jelly that fills the eye pulls away from the retina as part of normal ageing. The concern is that in roughly one in ten people with these sudden symptoms, the pulling jelly tears the retina. A retinal tear can be sealed with laser treatment if it is found early. Left alone, it can lead to a retinal detachment, which is far more serious.

A retinal detachment can also show up as a sudden shadow or curtain. If it is caught before it reaches the macula, surgery has a much better chance of saving central sight. A sudden shower of new floaters with flashing lights should be checked within a day.
3. A Red Eye That Overstays Its Welcome
A red eye is one of the most common reasons people see a doctor, and most causes are harmless. These usually clear within a couple of weeks.
Redness that lasts longer than two weeks, or that comes with pain, light sensitivity or reduced vision, especially in one eye, needs a specialist assessment. One important cause is anterior uveitis, inflammation inside the front of the eye, which can raise the pressure in the eye and lead to lasting damage if untreated. Uveitis is sometimes linked to conditions elsewhere in the body, such as certain types of arthritis or bowel inflammation. A rarer but serious cause is scleritis, a deep inflammation of the white of the eye. It is usually very painful, tender to touch, and needs prompt specialist care.
4. When Straight Lines Start to Bend
If straight lines look wavy, curved or broken when you look with one eye, this usually points to a problem at the macula, the central part of the retina that gives sharp, detailed vision.
The most common cause in older adults is age-related macular degeneration (AMD). In the wet form, fragile new blood vessels grow under the retina and leak fluid or blood. Wet AMD can be treated with injections that help protect sight, but the treatment works best when started quickly, ideally within days of symptoms beginning. If you are over fifty, and especially if you smoke or have a family history of AMD, new distortion in your central vision should be checked within a day or two.
5. The Glaucoma Emergency People Miss
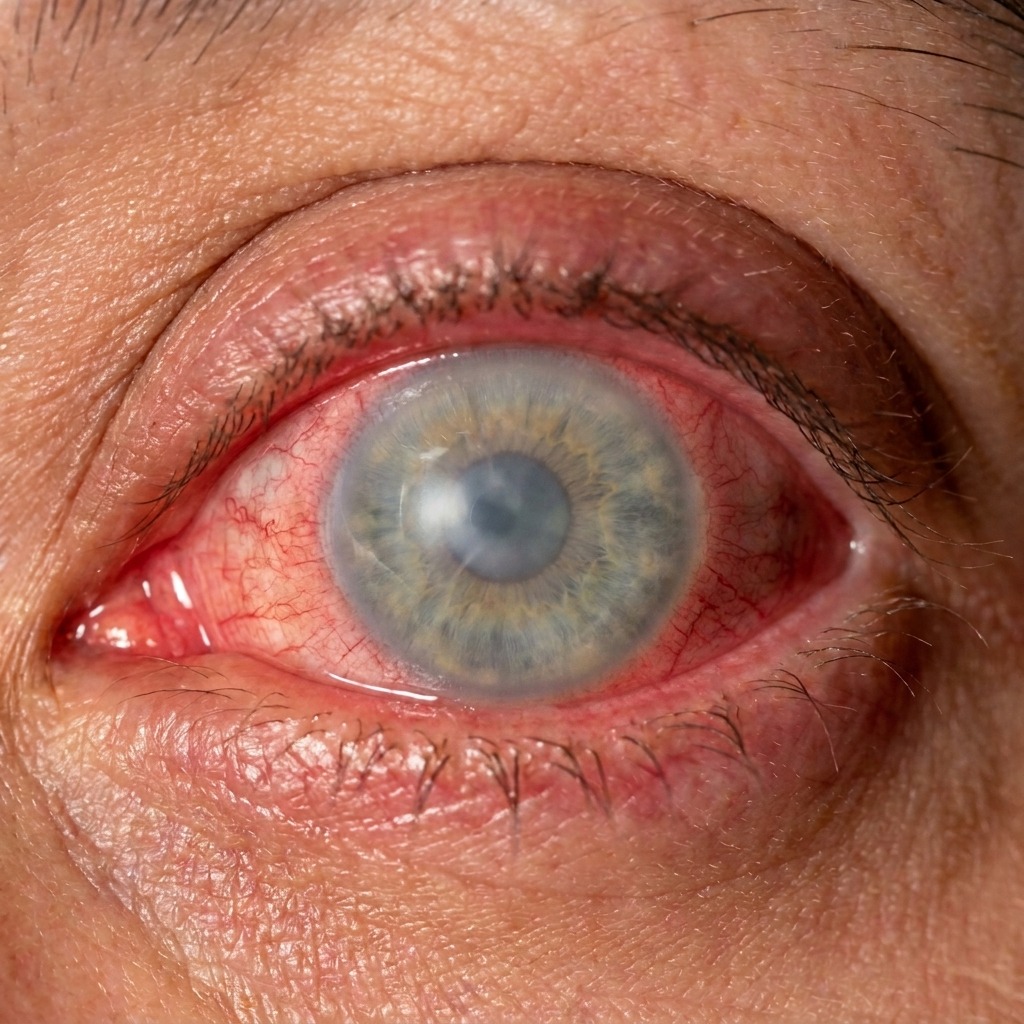
In acute angle-closure glaucoma, the eye's drainage system blocks quickly and the pressure inside the eye rises sharply. It causes severe pain in and around one eye, often with headache, feeling sick or vomiting, blurred vision due to cloudy cornea, compression of the nerve in the eye, a dilated pupil, and a red eye. Because the headache and nausea can be so strong, this is sometimes mistaken for a migraine or a stroke and patients are wrongly investigated with brain imaging whilst precious time is passing with high pressure in the eye risking permanent damage to vision. If you have sudden severe eye pain with nausea and a red eye, go straight to an emergency eye service.
Knowing How Quickly to Act
The table below is a simple guide to how urgently each symptom usually needs attention. It is a starting point, not a diagnosis. If you are unsure, it is always reasonable to ask for advice.
References
- Royal College of Ophthalmologists. Retinal artery occlusion: clinical guidance. London: RCOphth.
- Royal College of Ophthalmologists. Management of acute retinal detachment: clinical guidance. London: RCOphth.
- Mackie SL, Dejaco C, Appenzeller S, et al. British Society for Rheumatology guideline on diagnosis and treatment of giant cell arteritis. Rheumatology (Oxford). 2020;59(3):e1-e23.
- American Academy of Ophthalmology. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration: Preferred Practice Pattern. San Francisco: AAO.
- National Institute for Health and Care Excellence. Cataracts in adults: management. NICE Guideline NG77. London: NICE; 2017.
- Godefrooij DA, de Wit GA, Uiterwaal CS, Imhof SM, Wisse RPL. Age-specific incidence and prevalence of keratoconus: a nationwide registration study. Am J Ophthalmol. 2017;175:169-172.
- American Academy of Ophthalmology. Uveitis: Preferred Practice Pattern. San Francisco: AAO.
- American Academy of Ophthalmology. Scleritis: clinical overview (EyeWiki). San Francisco: AAO.
- National Institute for Health and Care Excellence. Age-related macular degeneration. NICE Guideline NG82. London: NICE; 2018.
- American Academy of Ophthalmology. Idiopathic Epiretinal Membrane and Vitreomacular Traction: Preferred Practice Pattern. San Francisco: AAO.
- National Institute for Health and Care Excellence. Glaucoma: diagnosis and management. NICE Guideline NG81. London: NICE; 2017 (updated 2022).
- Royal College of Ophthalmologists. The acute red eye and ocular emergencies: clinical guidance. London: RCOphth.
- Herpetic Eye Disease Study Group. Oral acyclovir for herpes simplex virus eye disease: effect on prevention of recurrent disease. N Engl J Med. 1998;339(5):300-306.
- Tear Film and Ocular Surface Society. TFOS DEWS III Report. The Ocular Surface; 2025.
